Postnatal Return to Running – A Framework for Health Professionals

As health professionals supporting women following birth, we often find ourselves being asked “when can I return to running – it’s the form of exercise that works best for me.” In the back of our minds is wanting to prevent the occurrence of the statistic we all know well - 1 in 3 women will experience pelvic floor dysfunction after childbirth. So how to do balance these potentially conflicting situations? This challenge has led to women receiving inconsistent and conflicting advice about postpartum exercise. This has not only reduced engagement in physical activity but has left both new mothers and health professionals navigating uncharted territory.
Without national or international guidelines, clinicians often default to generalised recommendations or arbitrary timelines. These approaches fail to address the complex physiological, biomechanical, and psychological changes unique to the postpartum period, leaving women without appropriate, evidence-based support for safely resuming activities like running.
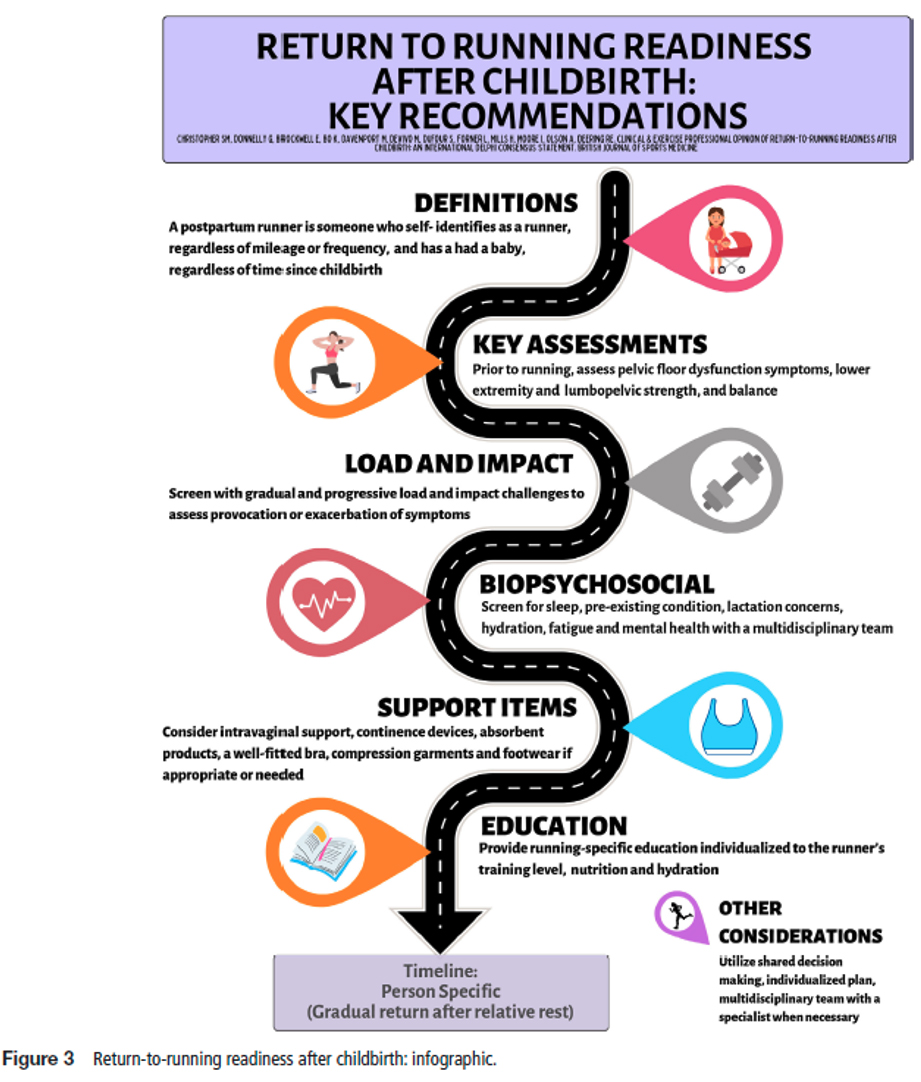
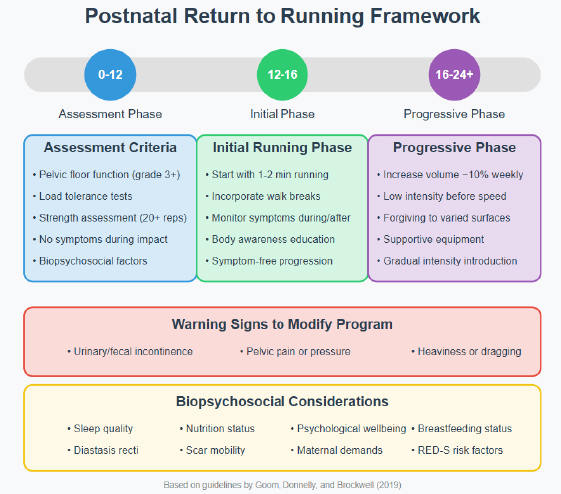 Addressing the large research gap in postpartum exercise, Physiotherapists Tom Goom, Grainne Donnelly and Emma Brockwell1 developed evidence-based guidelines that enhance clinical reasoning for practitioners. These guidelines serve as a foundation for future standardised protocols supporting safe return to running after childbirth.
Addressing the large research gap in postpartum exercise, Physiotherapists Tom Goom, Grainne Donnelly and Emma Brockwell1 developed evidence-based guidelines that enhance clinical reasoning for practitioners. These guidelines serve as a foundation for future standardised protocols supporting safe return to running after childbirth.Recommendation 1: The Need for Individualised Assessment and Rehabilitation
- Urinary or faecal incontinence
- Difficult-to-defer urinary or faecal urgency
- Pelvic heaviness, pressure, bulging, or dragging sensations
- Pain during intercourse
- Obstructed defecation
- Pendular abdomen, separated abdominal muscles, or decreased core strength
- Musculoskeletal lumbopelvic pain
Recommendation 2: Return to running is not advisable before 3 months
- Pelvic Floor Structure: The levator hiatus widens during pregnancy and expands significantly after vaginal delivery. While it improves by 12 months postpartum, it rarely returns to pre-pregnancy size. Optimal recovery of the levator ani muscle and supporting tissues occurs by 4-6 months.
- Bladder Support: Bladder neck mobility increases following vaginal delivery and remains higher than pregnancy levels even after recovery.
- Cesarean Recovery: Ultrasound studies reveal the uterine scar remains thickened at 6 weeks, indicating ongoing healing. Abdominal fascia regains only 51-59% of its original strength by 6 weeks, improving to 73-93% by 6-7 months postpartum.
- Pelvic heaviness/dragging (possible prolapse)
- Urinary leakage or bowel control issues
- Pendular abdomen or midline gap (possible diastasis recti)
- Pelvic/lower back pain
- Abnormal bleeding beyond 8 weeks postpartum
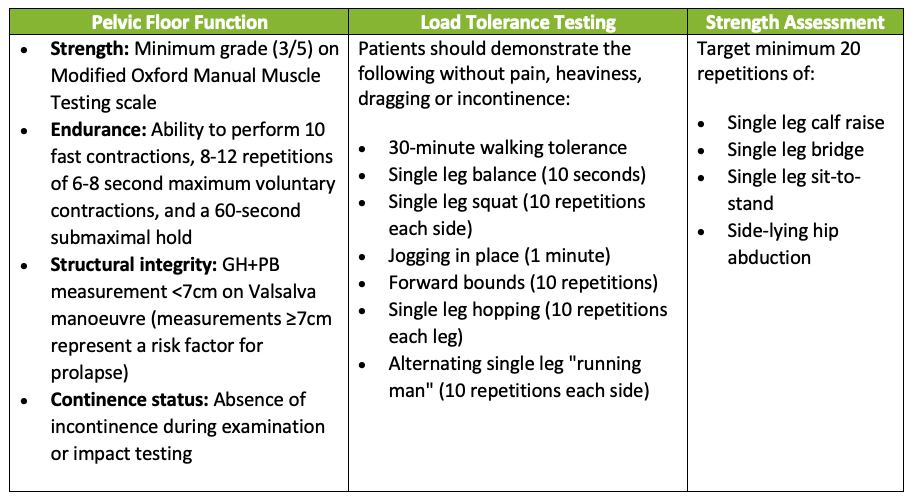
Recommendation 3: Before assessing readiness to run assess your patients pelvic floor health, load management and strength.
Recommendation 4: Whole-Person Considerations
- Weight status: BMI >30 increases risk of pelvic floor dysfunction and musculoskeletal injuries.
- Diastasis Recti: Screening for Diastasis Recti Abdominis (DRA), the separation of the outermost abdominal muscles, is recommended by qualified professionals like pelvic health physiotherapists, as DRA can impact abdominal wall function. While research on running with DRA is limited and its relationship with pelvic floor dysfunction remains debated, expert consensus suggests that running before regaining functional control of the abdominal wall may be counterproductive, potentially leading to overloading or compensatory strategies in the pelvic floor.
- Psychological Status: Screen for postnatal depression using the Edinburgh Postnatal Depression Scale.
- Scar Mobilisation: Consideration of scar mobility and mobilisation is important regardless of delivery method, as both c-section and perineal scars can cause pain and restriction by altering tissue dynamics and potentially affecting adjacent muscles and organs. Scar mobilisation is recommended as good practice since it may reduce inflammation and fibrosis while improving tissue remodelling.
- Breastfeeding Status: Consider potential effects on joint laxity due to hormonal influences, mainly reduced oestrogen levels. Education should be provided about timing of feeds around running, to ensure that the breasts are not overly full or likely to become uncomfortably full during the run.3
- Sleep Quality: Assess for sleep deprivation, which can increass injury risk and recovery.
- Relative Energy Deficiency in Sport (RED-S): RED-S refers to impaired physiological functioning caused by inadequate energy intake relative to expenditure, affecting metabolic rate, menstrual function, bone health, immunity, and cardiovascular health. Postnatal women may be particularly vulnerable to RED-S due to breastfeeding demands, social pressure to regain pre-pregnancy fitness, and compromised nutrition, which can impact psychological wellbeing, bone health, pelvic floor function and fertility, requiring education and screening when returning to running. Screen for signs of energy deficit using the RED-S Clinical Assessment Tool.
- Supportive clothing: Okayama et al.4 showed that wearing supportive underwear was nearly as effective as pelvic floor muscle training in reducing stress urinary incontinence in women after a 6-week trial. Further high-quality studies are needed to assess how each intervention compares over a longer period beyond 6 weeks.
Moving Forward